
Introduction: Beyond the "Mom Pooch" – Understanding Abdominal Separation
Section 1: What is Diastasis Recti? A Structural Perspective
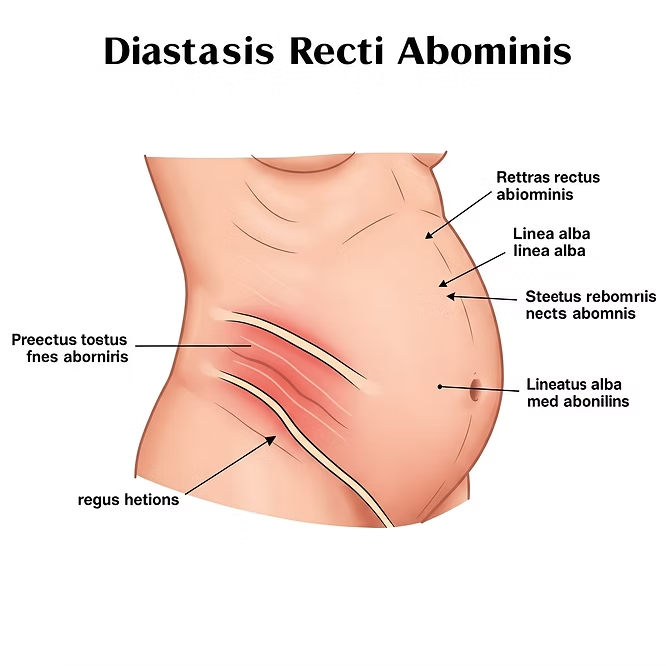
Anatomy of the Abdominal Wall
The rectus abdominis (“six-pack” muscles) are two parallel muscle bands connected by the linea alba, a fibrous midline structure. Under excessive intra-abdominal pressure, this tissue thins and stretches, creating a gap—typically measured at the umbilicus, above, or below.
Clinical Definition
A separation of ≥2.7 cm (about two finger-widths) is generally diagnostic, though functional deficits (core weakness, doming) matter more than the gap size alone.
Who Develops Diastasis Recti?
Population | Prevalence | Contributing Factors |
Postpartum women | 30-60% | Hormonal changes, fetal growth, delivery |
Men | 10-15% | Obesity, heavy lifting, poor exercise form |
Newborns | Common | Prematurity, weak abdominal musculature |
Section 2: Causes and Pathophysiology – Why Does It Happen?
Primary Mechanisms
1. Hormonal Influence
- Relaxin and progesterone increase ligamentous laxity, reducing linea alba tensile strength.
2. Mechanical Overload Pregnancy: - The expanding uterus exerts ~20-40 mmHg pressure on the abdominal wall.
- Chronic straining (e.g., constipation, COPD) repetitively stresses the midline.
3. Faulty Movement Patterns - “Open-scissor” posture (rib flare + anterior pelvic tilt) exacerbates separation.
- Compensatory strategies (e.g., breath-holding during lifts) spike intra-abdominal pressure.
High-Risk Scenarios - Multiparous pregnancies (risk increases with each birth)
- Macrosomia (large baby >4 kg)
- Polyhydramnios (excess amniotic fluid)
- Poorly managed intra-abdominal pressure (e.g., CrossFit, weightlifting without core coordination)
Section 3: Complications of Untreated Diastasis Recti
Musculoskeletal Consequences
- Lumbar instability → Chronic low back pain (78% of DR patients report this)
- Pelvic floor dysfunction → Stress incontinence, prolapse
- Reduced athletic performance → Compromised force transfer in running, lifting
- Aesthetic and Functional Concerns
- Abdominal doming (visible bulge during exertion)
- Failed traditional ab workouts (crunches widen the gap)
Section 4: Physiotherapy Management – A Stepwise Approach
Phase 1: Motor Control Re-Education (Weeks 1-6)
Goal: Restore neuromuscular connection to the transverse abdominis (TVA) and pelvic floor.
Key Exercises:
1. Diaphragmatic Breathing
- Supine, knees bent. Inhale to expand ribs laterally, exhale to engage TVA + pelvic floor.
- Cue: “Imagine zipping up a tight pair of jeans from pelvis to ribcage.”
2. Pelvic Tilts - Gentle posterior tilts to activate deep core without straining linea alba.
3. Heel Slides - Maintain TVA engagement while sliding one leg out slowly.
Phase 2: Progressive Loading (Weeks 6-12)
Key Exercises:
1. Dead Bug Progression Start with bent knees → progress to straight legs as control improves.
2. Side-Lying Clamshells Strengthen obliques to support midline closure.
3. Standing Pallof Press Anti-rotation training to reinforce core stability.
Phase 3: Functional Integration (3+ Months)
Advanced Techniques:
- Ballistic movements (e.g., medicine ball throws) with exhale bracing
- Dynamic planks (only if no doming occurs)
When to Refer for Surgical Consultation - Gap >4 cm persisting beyond 12 months of rehab
- Symptomatic ventral hernia
- Severe functional limitations (e.g., inability to perform ADLs)
Conclusion: A Call to Action
Diastasis recti isn’t just a cosmetic concern—it’s a functional deficit requiring targeted rehab. As physiotherapists, our role is to:
1. Educate patients on pressure management.
2. Prescribe individualized, progressive programming.
3. Empower long-term core resilience.
For Clinicians: Always assess DR in postpartum and athletic populations—it’s frequently missed!
For Patients: Skip the crunches. Start with breath work, and commit to the process. Your core can recover.
